La actinic cheilitis affects the 31.3% of the population over 45 years of age in Spain, according to a multicenter study conducted in our country [(Rodriguez-Blanco et al., 2018)]. It is a premalignant lesion of the lip caused by chronic sun exposure that, if left untreated, can progress to squamous cell carcinoma.
Have you ever noticed that your lower lip is always dry, chapped, or has a rough texture that doesn't improve with lip balms? It may not just be dryness. Here's everything you need to know to identify, treat, and prevent it.
My name is Sebastian Podlipnik and I am Dermatologist at the Melanoma and Skin Cancer Unit of Hospital Clínic de Barcelona. In my clinical practice, I frequently see patients with actinic cheilitis who did not know they had a premalignant lip lesion. Many come in thinking it is simply dry skin. That is why I believe information is the best tool for prevention.

What will this article cover?
- What is actinic cheilitis?
- Why does it affect the lower lip more?
- What are the symptoms?
- Is actinic cheilitis cancer?
- Difference with actinic keratosis
- How is it diagnosed?
- What is the best treatment?
- Prevention and lip sun protection
- Frequently Asked Questions
What is actinic cheilitis?
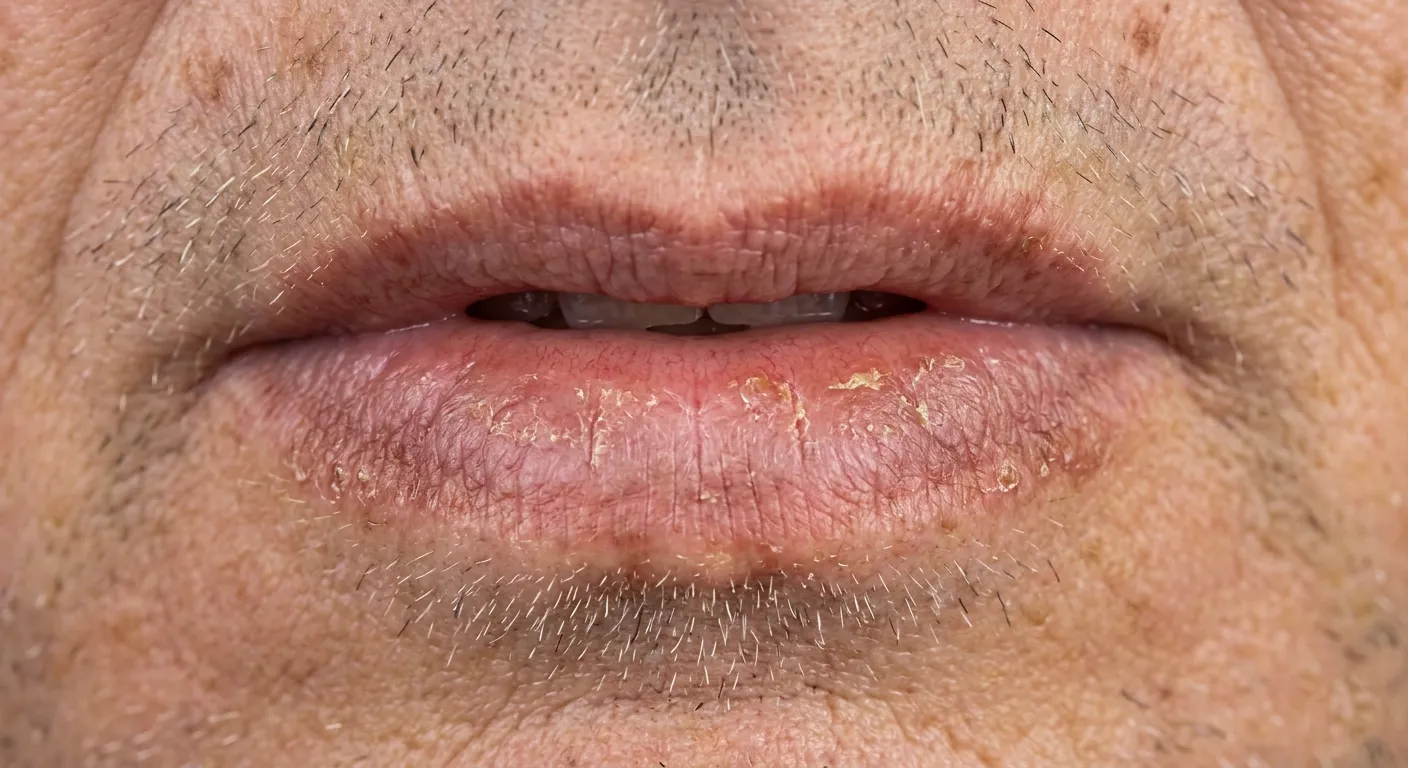
Actinic cheilitis is a potentially malignant lip disorder caused by cumulative exposure to ultraviolet radiation from the sun. It manifests as chronic changes in the lip mucosa (persistent dryness, scaling, loss of the well-defined vermilion border) and predominantly affects the lower lip.
An international consensus of experts, led by Warnakulasuriya, classified this lesion as a "potentially malignant disorder" with the highest consensus score (median 7 out of 7), stressing that it requires histopathological confirmation for proper management. [(Seoane et al., 2021)].. Unlike simple dry lips, actinic cheilitis represents cumulative solar damage to the lip cells that, over time, can progress to squamous cell carcinoma, the second most common type of skin cancer. It is not a condition that can be resolved with moisturizers or lip balms. It requires dermatological evaluation, follow-up, and, in many cases, active treatment to prevent progression. The good news is that, when detected early, it has multiple therapeutic options with success rates higher than 75%.
- Actinic cheilitis
- Premalignant lesion of the lip caused by chronic sun damage. It is classified as a potentially malignant disorder that can progress to squamous cell carcinoma if left untreated.
Why does it affect the lower lip more?
The lower lip receives ultraviolet radiation directly because it faces upward, exposed to the sun like a "little terrace" on your face. The upper lip, on the other hand, is partially protected by the shadow of the nose. In addition, the lip mucosa has less melanin than the rest of the skin, which makes it more vulnerable to UV damage.
A 10-year retrospective study confirmed that the 87.6% of the patients with this condition had occupational sun exposure. The most affected professions are: farmers, construction workers, fishermen and outdoor sportsmen. [(Pierin et al., 2024)].. The typical profile is a man (67.8% of cases) over 60 years of age with a light phototype (skin that burns easily). A multicenter study conducted in northwestern Spain identified as independent risk factors: age 60 years or older, Fitzpatrick phototype II, working outdoors for more than 25 years, and a personal history of non-melanoma skin cancer. [(Rodriguez-Blanco et al., 2018)]. However, anyone with chronic sun exposure can develop it, regardless of their profession.
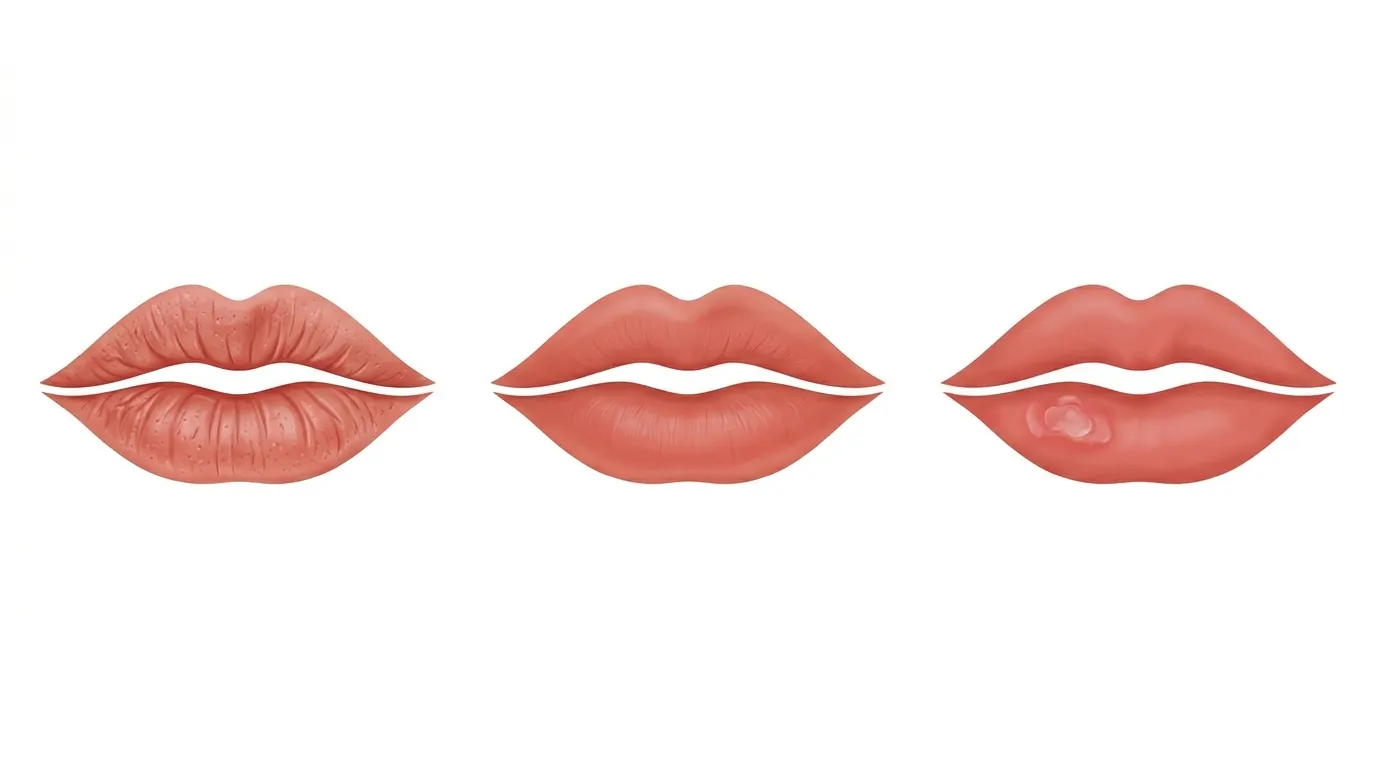
What are the symptoms?
The main symptoms are persistent dryness of the lip (99% of cases), effacement of the vermilion-skin border (82%), desquamation (69%) and atrophy of the lip (69%), according to a meta-analysis that analyzed data from multiple clinical studies. [(Carneiro et al., 2023)].. Unlike common dry lips, these symptoms do not improve with lip balms or moisturizing and persist for weeks or months. The same study found that mild dysplasia was present in 34.2% of cases, moderate dysplasia in 27.5% and severe dysplasia in 14.9%, confirming that this lesion can present different degrees of cellular alteration that determine both the prognosis and the most appropriate treatment.

I recommend that you pay attention to the following signs, organized by severity:
| Severity | Clinical signs | What to do |
|---|---|---|
| Slight | Persistent dryness, rough lip to the touch, fine scaling | Scheduled dermatological consultation |
| Moderate | Blurring of the lip border, white spots or erythema, atrophy | Priority dermatological consultation |
| Severa | Non-healing ulcers, indurated areas, spontaneous bleeding, palpable lump | Urgent consultation (possible malignant transformation) |
If you detect any of these signs on your lip, especially if you have been exposed to the sun for years without lip protection, I recommend that you consult a doctor. dermatologist specializing in skin cancer.
Do you need an appraisal? Request an online visit or a on-site visit in Barcelona.
Is actinic cheilitis cancer?
No, it is not cancer, but it is a premalignant lesion.. This means that the lip cells already show sun damage (dysplasia) but have not yet transformed into a carcinoma. If left untreated, the risk of transformation to squamous cell carcinoma (the second most common type of lip carcinoma) is higher. skin cancer) is considerable.
Data on the exact rate of malignant transformation vary among studies. A review published in Frontiers in Medicine placed the range between 10% and the 30% [(Vasilovici et al., 2022)].. A more recent meta-analysis estimated a rate of 14% [(Carneiro et al., 2023)]., while a retrospective 10-year study documented a malignant transformation in the 12.05% of the 224 patients followed [(Pierin et al., 2024)].. What these data clearly tell us is that between 1 in 7 and 1 in 10 patients with this untreated lesion will develop lip cancer. And what makes this especially worrisome is that lip squamous cell carcinoma has a much higher rate of metastasis than the same tumor in other skin sites.
"Actinic cheilitis is a warning signal your lip is sending you. Detecting it early makes the difference between a simple treatment and a much more complex problem."
Dr. Sebastian Podlipnik
What is the difference between actinic cheilitis and actinic keratosis?
Actinic cheilitis is essentially the lip version of the actinic keratosis. Actinic keratoses are rough, scaly patches that appear on areas of skin exposed to the sun (face, scalp, hands, forearms). Both lesions are premalignant, are caused by accumulated sun damage and share the same mechanism: ultraviolet radiation damages the DNA of cells, generating dysplasia that can progress to squamous cell carcinoma.
The main difference is the location and its clinical implications. The mucosa of the lip is thinner and has fewer natural defenses against the sun (less melanin, less thickness) than the skin of the rest of the body. This means that the lip lesion may behave more aggressively. If you have been diagnosed with actinic keratoses If you have sun damage on your face or scalp, it is very likely that your lip has also received sun damage and should be checked.
How is it diagnosed?
The diagnosis is made by clinical examination, dermatoscopy and, when indicated, biopsy. Your dermatologist will examine the lip for the characteristic signs: chronic dryness, loss of vermilion border, whitish or erythematous areas, and areas of atrophy or induration.
La dermatoscopy allows examination of the lip under magnification and polarized light, identifying vascular and structural patterns that guide the diagnosis without the need for biopsy in all cases. The international consensus of experts established that the histopathological confirmation is mandatory to define the degree of dysplasia and to guide treatment [(Seoane et al., 2021)].. This means that, in most cases, I will recommend that you perform a small biopsy of the lip to analyze the tissue under a microscope.
- Dysplasia
- Alteration of cells indicating abnormal growth. It is classified as mild (34.2% of cases), moderate (27.5%) and severe (14.9%). The higher the degree of dysplasia, the greater the risk of malignant transformation.
If you want to know more about the importance of dermatological screening, I wrote an article on how to detect skin cancer early.
What is the best treatment?
The best treatment depends on the severity of the injury. A systematic review published in the JAAD documented a overall clinical complete response rate of 76.5%, with important differences according to the therapeutic modality. [(Lai et al., 2020)].. Treatments are divided into surgical and non-surgical.
Non-surgical treatments
- Photodynamic therapy (PDT): a treatment that uses a photosensitizing cream and a light source to selectively destroy damaged cells. The photodynamic therapy conventional achieves full response of the 65-69% [(Yang et al., 2022)].. There is a daylight variant that is significantly less painful: the 87.10% of patients report no pain., compared to 31,25% with conventional PDT.
- Imiquimod 5% (cream): a topical immunomodulator that activates the body's defenses against abnormal cells. The most recent meta-analysis attributes to it the lower recurrence rate among all the options [(Al-Fartwsi et al., 2025)]..
- 5-Fluorouracil topical: a chemotherapeutic cream that destroys fast-growing cells. Effective but with local side effects (inflammation, crusting) during the weeks of treatment.
- Topical diclofenac 3%: a better tolerated option but with lower efficacy (clearance rate of 53%).
Surgical treatments
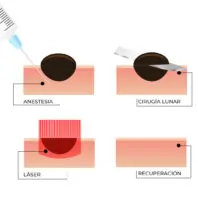
- CO2 laser: vaporizes the superficial layers of the affected lip. It is the treatment with highest clearance rate: 93.8-97% [(Lai et al., 2020)]. [(Al-Fartwsi et al., 2025)]..
- Vermellonectomy: surgical removal of the entire mucosa of the affected lip (vermilion). It is the most radical treatment, with a response rate of 100%, but involves a longer postoperative period.
- Cryotherapy: destruction of lesions by extreme cold (liquid nitrogen). Useful for localized lesions.
A meta-analysis that directly compared the two approaches found that the surgical treatments achieve 92.8% remission vs. 65.9% for non-surgical treatments., with a lower recurrence rate (8.4% vs. 19.2%). [(Carvalho et al., 2018)].
| Treatment | Complete answer | Recurrence | Main advantage |
|---|---|---|---|
| CO2 laser | 93.8-97% | Download | Increased overall efficiency |
| Vermellonectomy | 100% | Very low | Definitive, allows complete histological analysis |
| Conventional PDT | 65-69% | Moderate | Non-invasive, good aesthetic result |
| TFD daylight | 76.7% | Moderate | Painless (87% of patients) |
| Imiquimod 5% | Moderate | Very low | Lower recurrence |
| 5-Fluorouracil | Moderate | Moderate | Accessible, domiciliary |
Do you need an appraisal? Request an online visit or a on-site visit in Barcelona to evaluate your case and recommend the most appropriate treatment.
How to prevent actinic cheilitis? Lip photoprotection
Prevention is based on daily lip photoprotection with a lip balm with SPF 30 or higher. It is the simplest and most effective measure, yet it is the most overlooked: more than 90% of patients diagnosed with actinic cheilitis had never used sunscreen on their lips. [(Rodriguez-Blanco et al., 2019)].
I recommend that you follow these prevention guidelines:
- Use a lip balm with SPF 30+ daily., even on cloudy days and in winter. Reapply every 2 hours if you are outdoors.
- Wear a wide-brimmed hat to protect the face and lips from direct radiation.
- Avoid sun exposure in the central hours (12:00-16:00), especially if you work outdoors.
- Do not use tanning beds. UVA radiation from tanning beds also damages the labial mucosa.
- Check your lips periodically. If you notice persistent dryness, texture or color changes that do not improve in 2-3 weeks, consult your dermatologist.

If you want to learn more about sun protection, I recommend my article on sunscreens. best sunscreens. In addition, the nicotinamide (vitamin B3) has proven to be a useful adjunct in the chemoprevention of actinic lesions.
Frequently asked questions about actinic cheilitis
Is actinic cheilitis cured?
Yes, actinic cheilitis can be successfully treated. The complete response rate varies from 65% to 97% depending on the treatment chosen. CO2 laser offers the best cure rates (93.8-97%), while topical treatments such as photodynamic therapy or imiquimod are less invasive options with good results. Your dermatologist will recommend the most appropriate option according to the severity of your case.
What happens if I do not treat actinic cheilitis?
Without treatment, there is a risk of transformation to squamous cell carcinoma of the lip estimated between 10% and 14% according to the most recent meta-analyses. This means that approximately 1 in 7-10 patients with untreated actinic cheilitis will develop lip cancer. Early detection and treatment is the best strategy to prevent this progression.
Can actinic cheilitis return after treatment?
Yes, recurrence is possible because the accumulated sun damage does not disappear. The recurrence rate varies from 8.4% in surgical treatments to 19.2% in non-surgical treatments. Therefore, after treatment, you need to maintain daily lip photoprotection and have regular check-ups with your dermatologist.
Which physician treats actinic cheilitis?
A dermatologist is the specialist indicated to diagnose and treat actinic cheilitis, preferably with expertise in premalignant lesions and skin cancer. Although some cases are referred by dentists or odontologists, the definitive management corresponds to the dermatologist, who has the necessary diagnostic (dermatoscopy, biopsy) and therapeutic tools.
Does lip sunscreen prevent actinic cheilitis?
Yes, regular use of a lip balm with SPF 30 or higher is the most important preventive measure. The most revealing data is that more than 90% of patients with actinic cheilitis had never used lip photoprotection. Incorporating this habit into your daily routine, along with wearing a hat and avoiding sun exposure in the middle of the day, significantly reduces the risk.
Consultation with a specialist dermatologist
Actinic cheilitis is a premalignant lesion that deserves professional attention. Fortunately, detected early it has an excellent prognosis and multiple effective treatment options. If you have noticed persistent changes in your lips, or if you work outdoors and have never checked this area, don't wait.
"Your lips need sun protection, too. A simple balm with SPF can be the difference between prevention and a diagnosis no one wants to receive."
Dr. Sebastian Podlipnik
Request your visit: Online visit | On-site visit in Barcelona