If you've arrived here looking for "itchy mole," you're probably experiencing anxiety. And it's important to clarify from the outset: most itchy moles are benign. However, itching can, under certain circumstances, be a sign to take seriously. Knowing when it matters and when it doesn't is what saves you months of worry or, in some cases, a life-changing visit.
In this article, I'll explain, with verifiable scientific data and a real case from my practice, when an itchy mole warrants a check-up and when you can rest easy.
My name is Sebastian Podlipnik and I am Dermatologist at the Melanoma and Skin Cancer Unit of Hospital Clínic de Barcelona. I've been treating patients for years who come into my office with this same question. That experience, combined with the evidence we're about to review, is the foundation for what you're about to read.
When is mole itching a sign of melanoma?
Itching in a mole is a warning sign when it persists for more than two weeks and is accompanied by visible changes: asymmetry, irregular borders, heterogeneous color, growth, bleeding, or crusting. Most itchy moles are benign. Isolated itching, without visual changes, rarely indicates melanoma.
This contradicts a widely held popular belief: the idea that "itchy mole = melanoma." The clinical reality is more nuanced. A prospective study of 339 skin cancers showed that itching is present in 36.9% of malignant lesions, but In melanomas, itching and pain were mostly absent. (Yosipovitch et al, 2014)
The clinical message you need to take away is twofold. First, don't panic if a mole itches one day and the next it doesn't. Second, don't get complacent thinking, "if it doesn't hurt or itch, it's nothing": melanoma can be completely asymptomatic. The useful rule is Itch matters when it's accompanied, not when he goes alone.
Why do moles itch? The 6 most common causes
Moles itch for very diverse reasons, and most have nothing to do with cancer. The itching comes from the superficial layers of the skin, where inflammatory mediators such as histamine or interleukin-31 stimulate nerve endings. (Rowe and Yosipovitch, 2015)
These are the six causes I see most frequently in consultation, ordered from least to most benign:
Dryness and friction
The most frequent cause. Dry skin or clothing friction irritates the mole, causing temporary itching. It subsides with moisturizing and refraining from scratching.
Dermatitis on the nevus
Eczema or contact dermatitis that settles on or around the mole. The itching is diffuse, also affecting the surrounding skin, and usually improves with anti-inflammatory dermatological treatment.
Seborrheic keratosis
Benign lesion in people over 40-50 years old that many call a "mole" but it is not. It has a waxy, sticky appearance, rough to the touch, and usually itches when scratched. It is the most common confusion.
Dermatofibroma
Small, firm, benign nodule that frequently appears on the legs. It itches when irritated by shaving or friction. It has no malignant potential.
Dysplastic nevus
Atypical mole with irregular borders and heterogeneous color. May itch subtly. It is not cancer, but requires dermatological review to rule out progression.
Melanoma
The cause prompting the consultation but is the least frequent. Itching is only relevant when associated with visual changes of ABCDE: asymmetry, borders, color, diameter, or evolution.
The practical conclusion is that context is key. A mole that itches one afternoon and stops itching after moisturizing is almost always due to dryness or friction. A mole that itches continuously for weeks, in a person with several risk factors, warrants dermatoscopy. I will discuss the visual criteria that accompany itching in the next section.
The ABCDE-I Criteria: When Itching Matters
You've probably heard of the ABCDEs for spotting suspicious moles. It's the most commonly used tool for self-examination, but few people know that itching is officially recognized as part of the letter E. I'll explain how this system evolved and why the "I" for Itch deserves its own attention.
In 1985, two New York dermatologists, Robert Friedman and Darrell Rigel, proposed a four-letter mnemonic so anyone could check their moles at home: ABCD. Asymmetry, Borders, Color, Diameter. That rule, as elementary as it is practical, became a worldwide standard. (Friedman and Rigel, 1985)
Nineteen years later, in 2004, a review published in JAMA officially expanded the criterion to ABCDE, adding the "E" from Evolving (evolving). And here comes the nuance that almost everyone ignores: the letter E doesn't just refer to visual changes. It expressly includes symptoms How itching and sensitivity. (Abbasi et al, 2004)
"Doctors and patients with moles should be alert to changes (evolution) in size, shape, symptoms (itching, tenderness), surface (especially bleeding), and color nuances."
This is a point worth dwelling on. When you apply the ABCDE at home, you're not just looking for an ugly mole. You're looking for any change in the weather, including itching. That's why I often use the extended acronym ABCDE-I With my patients: Asymmetry, Irregular borders, Heterogeneous color, Diameter greater than 6 mm, Evolution, and Itch. The "I" is not a new criterion; it's the explicit recognition that the symptom counts.
No single criterion of the ABCDE-I solely diagnoses melanoma. What matters is the combinationItching plus asymmetry, itching plus color change, itching plus growth. If a mole itches you and you also visually notice any other signs, that's where the ABCDE rule for identifying suspicious moles It stops being self-exploration and becomes a reason for consultation.

How long should a mole itch before you see a doctor?
The rule of thumb I use in consultation is simple: More than two weeks of persistent itching or any visual signs of the ABCDEs accompanying the itching warrant a review.. Brief, intermittent itching without other changes is rarely a cause for concern.
This two-week rule isn't arbitrary. What matters in a mole isn't just how much it itches, but the novelty of the symptom. If you have a mole that has itched intermittently for years, without changing its appearance, it is almost always irritation from friction or atopic eczema. If a mole that had not previously shown symptoms begins to itch persistently, that novelty does warrant attention.
Consult your dermatologist if you fit any of these descriptions:
- It's been more than 2 weeks straight., without yielding to hydration of the area.
- The itching coincides with any visual changesasymmetry, borders, color, size, crusting, bleeding.
- Do you have a family history of melanoma or many atypical moles.
- The mole is in an area that's difficult to check. (back, scalp, folds) and you can't watch it well.
- Have you had skin cancer before Fair skin type with severe sunburns in childhood.
Do you need an appraisal? You can request a online visit and send pictures of the mole for an initial assessment, or book an appointment In-person visit in Barcelona if you need a dermatoscopy or excision.

Clinical case: a small, itchy mole on the leg
The case that has impacted me the most on this topic, I remember perfectly. I was attending to a patient whom we followed in consultation for a condition compatible with FAMMM syndrome, the acronym for Familial Atypical Multiple Mole Melanoma. I had a direct family history of melanoma and a lot of moles all over my body, several with atypical criteria.
FAMMM syndrome warrants close follow-up because about 5-10% of cutaneous melanomas are hereditary. Mutations in the gene CDKN2A, a tumor suppressor, are found in 20-40% of families with this pattern. (Lynch and Shaw, 2016)
In our patient, we combined in-person visits with Digital dermoscopy and body mappingA systematic photography technique that allows images to be compared over time and subtle changes to be detected. It is the most rigorous monitoring tool we have for people with many atypical moles.
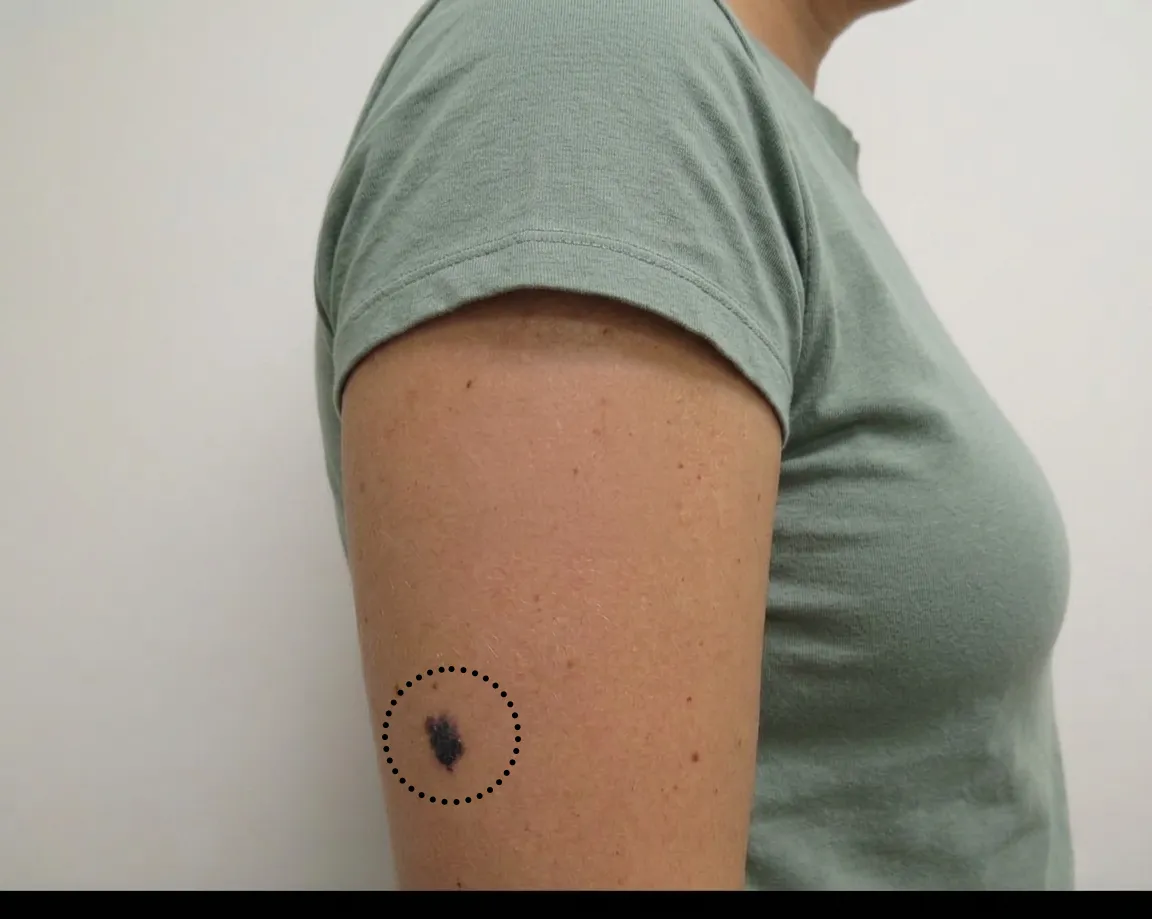
During a routine visit, he mentioned, almost in passing, that a small mole on his leg, hidden among others, had been itching him for a few weeks. It was a lesion of a few millimeters, with nothing striking to the naked eye. Without the itching symptom, we probably would have continued observing it at the next check-up.
Upon examination with the dermatoscope, despite its small size, it presented atypical criteria. We decided to excise it. The histopathological study confirmed Melanoma in situ: A melanoma confined to the epidermis, the outermost layer of the skin. The cure rate in these cases, with complete excision, approaches 100%. The patient is cured and continues with her follow-ups.
That story reminds me of something every time a patient comes into the office saying "Doctor, I have an itchy mole": the symptom can be the detail that changes the outcome. That's why I prefer to err on the side of caution and check one too many rather than ignore one too few.
Dr. Sebastian Podlipnik
Lunar mole that itches vs. seborrheic keratosis vs. dermatitis: how to distinguish them
Most inquiries about "itchy moles" do not result in a melanoma diagnosis. Most often, the lesion that prompts the visit isn't even a true mole, but one of three benign entities that are frequently mistaken for one. This table summarizes the key differences I evaluate during a consultation.
| Feature | Melanocytic nevus | Seborrheic keratosis | Dermatitis on nevus |
|---|---|---|---|
| Aspect | Flat or slightly raised spot, uniformly brown | Waxy, rough, "stuck" to the skin | Normal lunar with surrounding reddened skin |
| Typical age | Any age | From 40-50 years old | Any age, common in atopic skin |
| Picor | Rare and persistent if any | Frequent when scratching or rubbing | Diffuse, not focal on the mole |
| Evolution | Stable for years | It appears and grows slowly | Sprouts by environmental factors |
| When worried | If you change or meet ABCDE-I | When it suddenly appears in many areas (sign of Leser-Trélat) | If eczema persists despite topical treatment |
If your mole looks like a waxy blob and flakes off when you scratch it, it's most likely a seborrheic keratosis, a benign lesion that also itches. If the skin around the mole is red and itchy beyond the mole itself, it usually indicates dermatitis and warrants an evaluation to define the treatment. If the mole looks like a normal mole but is persistently itchy and you notice any subtle changes, it's time for a dermoscopy.
What do I do if a mole itches? At-home steps before seeing a doctor
Before panicking or scheduling an urgent appointment, there are three steps you can take at home that will give you useful information and help you make decisions. I recommend this simple protocol to all my patients.
- Moisturize the area and stop scratching. Apply a neutral moisturizing cream for 3-5 days. If the itching disappears, it was most likely dryness or chafing irritation.
- Photograph the mole with good light. Place a ruler or coin next to it for size reference. Take several photos from different angles. This photo will be your starting point for comparison.
- Rate the itch on a scale of 0-10. How many days has it been, subjective intensity, whether it's continuous or intermittent, and what triggers it. Having this record is more valuable than memory, especially during a consultation.
- Observe for 2 weeks. If after two weeks the mole still itches or you notice visual changes compared to the initial photo, it's time to consult.
- If you have a lot of moles, complement with a Monthly Self-Skin Exam Guide to review the rest.

When to see a dermatologist and what to expect from the appointment
If the mole continues to itch after two weeks, or if any visual sign of the ABCDE-I appears at any time, it's time to make an appointment. A dermatological consultation to evaluate a suspicious mole usually involves three steps: medical history, clinical examination, and dermatoscopy.
In the anamnesis, I will ask you about a family history of melanoma, phototype, sun exposure, childhood sunburns, previously removed moles, and the evolution of the current symptom. Therefore, bring your 0-10 record and photos. Five minutes of information from you is worth more than half an hour of blind exploration..
The exploration includes Digital dermatoscopy with full body mapping: a technique that allows visualization of dermal structures not visible to the naked eye and comparison of images over time. If you have many atypical moles, digital mapping becomes a key part of follow-up.

In some cases, we will request basic lab work, especially if the itching is diffuse (all over the body) and not focused on a specific mole. A complete blood count with differential, liver function, kidney function, thyroid function, and blood glucose levels help rule out systemic causes of itching. (Roh et al, 2022)
If dermoscopy shows atypical criteria, I will propose to you excision with biopsy. It is a quick office procedure, with local anesthesia, that removes the entire lesion for histological analysis. Results take between 7 and 15 days depending on the center. When dealing with an early-stage melanoma (thickness less than 0.76 mm), the prognosis is excellent. (Friedman and Rigel, 1985)
Frequently Asked Questions about Itchy Moles
Does an itchy mole always mean it's melanoma?
If my mole doesn't itch, does that mean it's not melanoma?
How long should a mole itch before I should worry?
What do I do if a mole itches and flakes?
Why do back moles itch?
Do I have a higher risk of melanoma if there's a family history?
Why did my dermatologist order blood tests for itching?
How do I describe itching to my dermatologist?
Do you have a mole that worries you? A timely assessment changes the outcome.
Online Visit On-site VisitReferences
- Yosipovitch G, Mills KC, Nattkemper LA, Feneran A, Tey HL, Lowenthal A, Pearce DJ, Williford PM, Sangueza OP, D'Agostino R Jr. Association of pain and itch with depth of invasion and inflammatory cell constitution in skin cancer: results of a large clinicopathologic study. JAMA Dermatology, 2014. PubMed
- Abbasi NR, Shaw HM, Rigel DS, Friedman RJ, McCarthy WH, Osman I, Kopf AW, Polsky D. Early diagnosis of cutaneous melanoma: revisiting the ABCD criteria. JAMA, 2004. PubMed
- Friedman RJ, Rigel DS. The clinical features of malignant melanoma. Dermatologic Clinics, 1985. PubMed
- Rowe B, Yosipovitch G. Malignancy-associated pruritus. European Journal of Pain, 2015. Wiley
- Sahu S, Yosipovitch G. Itch and pain in skin cancer. Clinics in Dermatology, 2021. ScienceDirect
- Roh YS, Choi J, Sutaria N, Kwatra SG. Itch: epidemiology, clinical presentation, and diagnostic workup. Journal of the American Academy of Dermatology, 2022. JAAD / ScienceDirect
- Lynch HT, Shaw TG. Familial atypical multiple mole melanoma (FAMMM) syndrome: history, genetics, and heterogeneity. Familial Cancer, 2016. Springer
- Gilli IO et al. Cutaneous melanoma diagnosis delay. Brazilian Medical Association Journal, 2022. PubMed