The Basal cell carcinoma is the most common human cancer, and also the one with the best prognosis.. It grows slowly, its spread to other organs is exceptional, and it is cured with appropriate surgery in the vast majority of cases. If you are reading this because you have been diagnosed with one, the first important thought is this: you are dealing with a very manageable tumor.
Basal cell carcinoma is a skin cancer with local behavior and an excellent prognosis. The vast majority resolve with simple surgery. Only a minority, almost always after years without treatment, become more complex, and even then, modern treatment is effective.
My name is Sebastian Podlipnik and I am Dermatologist at the Melanoma and Skin Cancer Unit of Hospital Clínic de Barcelona. I see basal cell carcinomas practically every week in my practice, and part of my job is the exact opposite of what the word "cancer" suggests: to reassure. In this article, I will explain, without opaque technicalities, what it is, the six ways it presents itself, and how each is treated.
Basal cell carcinoma is a type of skin cancer.
Basal cell carcinoma is the most common skin cancer and has the best prognosis. It originates from the basal cells of the epidermis (the deepest layer of the superficial skin) due to accumulated sun damage over the years. It grows slowly, locally, and almost never poses a risk to life.

The word "cancer" appearing is frightening, and rightfully so. That's why it's important to clarify something upfront: within the types of skin cancer, basal cell carcinoma is the most common and least aggressive, far from melanoma. "Carcinoma" and "cancer" are not different things: a carcinoma is a cancer that originates in epithelial cells, and in this case it is one of such indolent behavior that its real problem is not spreading, but that, if left untreated for a long time, it can damage neighboring tissue.
Basal cell carcinoma is the most common malignant tumor in fair-skinned individuals, and yet most resolve with a simple intervention. Its danger lies not in metastasis, which is exceptional, but in potential local destruction if ignored for years. That is the only real reason not to delay consulting with a doctor, and at the same time the best news: when detected early, which is usually the case, its management is straightforward and highly curative. (Kim et al., 2019)
A very frequent question in consultation is whether basal cell carcinoma comes from a actinic keratosis. The answer is no: unlike squamous cell carcinoma, basal cell it does not derive from actinic keratoses. It arises on its own, linked mainly to accumulated sun exposure and fair skin type. Knowing this avoids unnecessary alarm for those who have keratoses and fear they will "turn into" basal cell carcinoma.
Is it frequent? How many people does it happen to?
It is very frequent, and precisely that frequency is reassuring: you are not facing an alarming rarity, but rather the tumor that dermatologists see most and are best at resolving. In Spain, approximately 1 in 17 people will develop basal cell carcinoma in their lifetime, and the vast majority with very good outcomes.
This Spanish figure confirms something we had long suspected: basal cell carcinoma is much more common than older records suggested, because historically it was underreported due to its prevalence and low mortality rate. The study from Valencia, involving 2,171 patients and 4,047 tumors, also observed a sustained increase of approximately 3.91% annually, which was more pronounced in women. A Swedish population-based registry found figures of a similar magnitude, with a standardized incidence of 405 per 100,000 in 2017. (Kappelin et al, 2022)
Globally, the aging population leads to an increasing number of diagnoses, with millions of cases estimated in people over 65 years old. (Wang et al, 2025)
The fact that it's so common shouldn't be read as a threat, but quite the opposite: it's a daily tumor in dermatology, with a very established diagnostic and treatment path. The interesting question isn't "how many are there?" but "in what forms does it present and what do we do with each one?". That's what we're getting into.
The 6 faces of basal cell carcinoma: how to recognize each subtype
Not all basal cell carcinomas are the same, but the main idea is reassuring: the vast majority fall into the simpler management variants. Demanding faces are the minority. The subtype changes the appearance, growth rate, and treatment, and that's why it's worth knowing them, not to scare yourself, but to understand why each case is approached on a case-by-case basis.
European guidelines categorize basal cell carcinomas into "easy to treat," which are the vast majority, and "difficult to treat," which require a team approach. (Peris et al., 2023)
In my practice, I see this every day: the two most common forms are the nodular and infiltrative subtypes, which together account for about 31% of cases. (Kappelin et al, 2022)
Here are the six faces a dermatologist encounters, and you'll see that in all of them, when properly evaluated, the outcome is good.
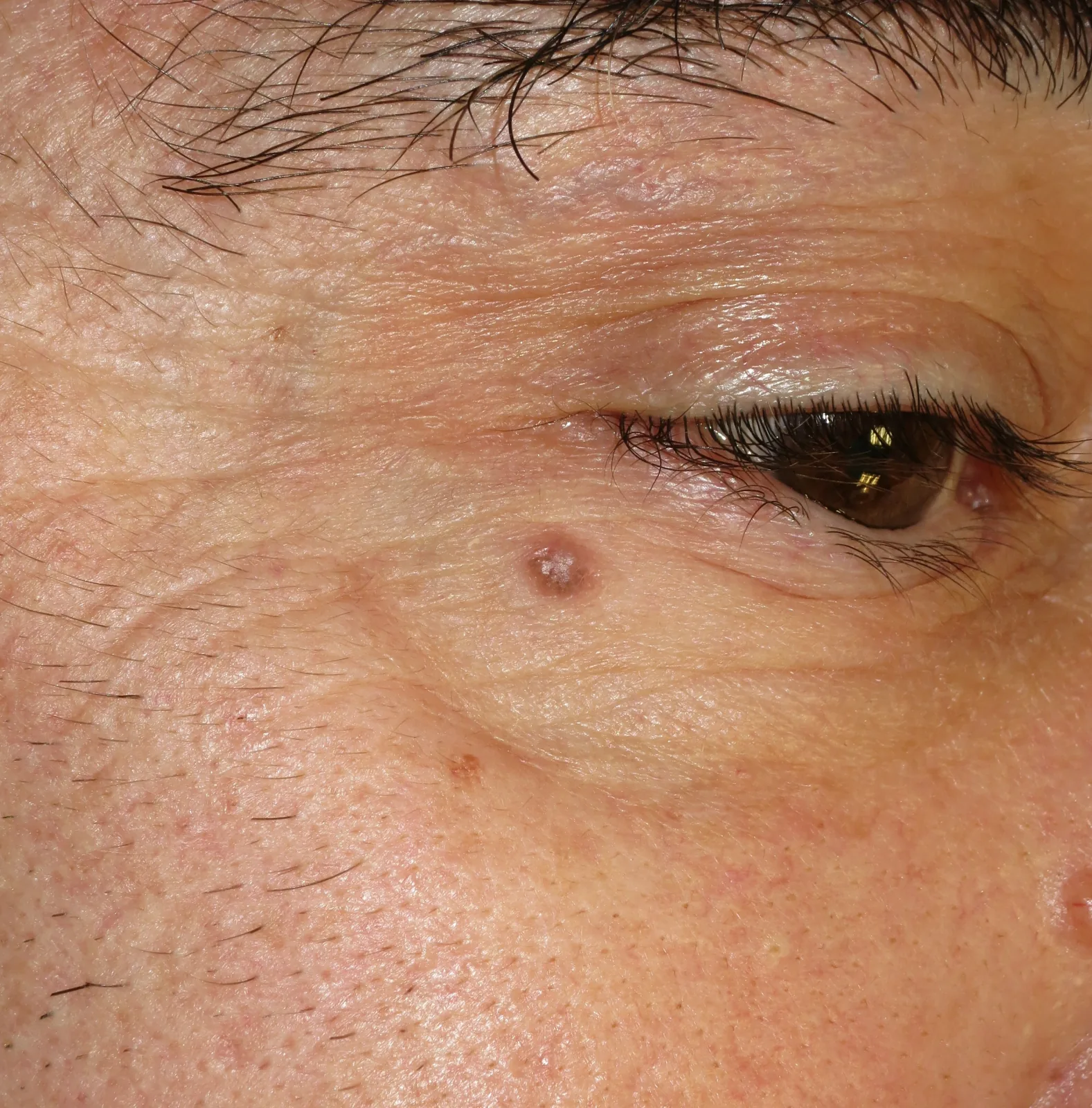
Nodular: the classic face
It is the most frequent and one of the easiest to handle. It appears as a Pearly, shiny, and translucent granite, often with fine blood vessels visible on the surface (telangiectasias) and sometimes a small central scab that comes and goes. It usually appears on the face. It's the "classic" face of basal cell carcinoma and the one a dermatologist recognizes best at a glance.
2. Superficial: the mildest
He/She/It presents himself/herself/itself as a Fine, slightly flaky reddish plaque, almost to the skin, often on the trunk. It is the least invasive variant and the one that responds best to treatments without a scalpel. It is often confused with eczema or psoriasis that "just won't go away" with moisturizing creams.

3. Pigmented: the one that imitates a mole
It's a basal cell carcinoma with brown or blue-gray pigment, so it can resemble an atypical mole, a melanoma, or a seborrheic keratosis. Here, peace of mind comes from a concrete tool: the dermatoscope distinguishes it very well from those other lesions, so the uncertainty of "what if it's something bad?" is usually resolved during the consultation itself.

4. Morpheiform or sclerodermiform: with a scar-like appearance
The morpheaform basal cell carcinoma (scar-like in appearance, poorly defined, also known as sclerosing) is the most intimidating type, and at the same time the rarest. A systematic review of 54 studies estimates that it accounts for only 5–10% of all basal cell carcinomas, meaning that approximately 90–95% of cases belong to variants that are easier to manage: the challenging cases are the exception, not the rule. (Conte et al, 2023)
5. Infiltrative or micronodular: ill-defined borders
It grows by infiltrating deeply, with less defined borders than the nodular type, so the dermatologist delimits it with special care. It remains a minority and, when assessed by a professional, also has a very good prognosis. The series that have characterized these aggressive variants work with small samples, which reminds us that they are the infrequent face of the tumor. (Gülseren et al, 2021)

6. Pinkus' Fibroepithelioma: The Uncommon One
It is an uncommon variant that usually appears as a pink papule or plaque on the lower lumbar area. It is included within the clinical spectrum of basal cell carcinoma, and despite its striking name, it has a favorable prognosis. (Di Stefani et al, 2015)
The important thing about this subtype map is the framing: the two most common types, nodular and superficial, are also the easiest to manage, and the more challenging ones are a minority that the dermatologist identifies and treats with good results. The following table summarizes each type with its frequency and usual approach.
| Cara | What does it look like | Frequency | Usual handling |
|---|---|---|---|
| Nodular | Pearlescent and shiny granite with small glasses | The most common (~31%) | Simple, very healing |
| Superficial | Thin reddish plaque on the trunk | Frequent | Offers non-surgical options |
| Pigmented | Pigmented lesion, mimics a mole | Variable | It is clearly distinguished with dermatoscopy. |
| Morphemic | Scarred hardened plate | Minority (5-10%) | Professional diligent evaluation |
| Infiltrator | Undefined edges, grows in depth | Minority | Careful delimitation, good prognosis |
| Pinkus's fibropithelioma | Pink papule on lumbar area | Rare | Favorable handling |
How is it diagnosed? The role of dermatoscopy
The dermatologist reliably identifies basal cell carcinoma without cutting the skin.. Suspicion is clinical and is confirmed with dermatoscopy, a lens with special light that reveals structures invisible to the naked eye, and only if there is doubt, with a biopsy. It is a quick, outpatient procedure, and almost always, reassuring.
La dermatoscopy It is a non-invasive technique that stretches the skin and eliminates its reflection, revealing blood vessels and pigment that aid in diagnosis. A meta-analysis of 17 studies found that it correctly detects basal cell carcinoma with a sensitivity of 91.21% and a specificity of 94.81%, and that adding the dermatoscope to simple visual inspection with the naked eye increases detection rates from 66.91% to 85.1%. Put simply, a handheld lens changes the diagnosis without a single incision, which is why it is advisable for a dermatologist to examine the lesion with a dermatoscope. (Reiter et al, 2019)

This is exactly the tool we use in the digital dermoscopy during the consultation. The dermatoscope doesn't just say, "This is a basal cell carcinoma"; it also identifies which subtype it is. A dermatoscopic algorithm distinguishes the superficial subtype from the others with a sensitivity of 81.91% and a specificity of 81.81%, meaning it correctly identifies the subtype in about 8 out of 10 cases. (Lallas et al, 2014)
For the more demanding variants, that same dermatoscope has its own repertoire of signs, such as thick branched vessels, porcelain-white areas, or small ulcerations, which guide the specialist even before considering a biopsy. (Camela et al, 2023)

Spanish dermatology has systematically detailed these patterns face by face, such that any trained dermatologist recognizes them reliably without needing to cut the skin. (Álvarez-Salafranca et al., 2021)
There is a statistic that helps explain why a specialist consultation is worthwhile, and it should be viewed as reassuring rather than alarming. To the naked eye, without a dermatoscope, the aggressive subtype is clinically diagnosed correctly in only about 22.1% of cases, compared to 86.21% for the nodular subtype and 49.91% for the superficial subtype. (Amici et al., 2021)
I see it often in my practice. Recently, a person came in with a small wound on the side of their nose that hadn't healed for months, which they attributed to their glasses rubbing. It was a nodular basal cell carcinoma and was resolved with a simple procedure. That's the most common story: a seemingly minor lesion that, when diagnosed in time, is easily treated.
The correct reading is not "how difficult it is," but: the uncertainty that the eye doesn't resolve, the dermatologist resolves with dermatoscopy. Therefore, if you see something new, changing, or, above all, on your skin, A wound or scab that doesn't completely heal, there's no need to be alarmed. It's simply time to ask for an evaluation. I'll explain when it's advisable to consult in the guide: early detection of skin cancer. If you prefer to clear up any doubts as soon as possible, you can resolve them in a online visit or, if you're in Barcelona, in a on-site visit.
How is each type of basal cell carcinoma treated?
Basal cell carcinoma is curable. Surgical excision is the gold standard treatment and resolves the vast majority of cases with very high cure rates. Depending on the subtype and location, the dermatologist chooses between excision, Mohs surgery, non-surgical options for superficial ones, or radiation therapy.
It's worth putting a specific figure on that peace of mind. Even in selected high-risk facial basal cell carcinomas, Nearly 9 out of 10 patients remain recurrence-free at 10 years with conventional excision surgery.. Healing is the norm, not the exception.
Conventional excision surgery, which involves removing the tumor with a small safety margin and then analyzing it in the laboratory, is the treatment of choice and works very well for the vast majority of basal cell carcinomas located in low-risk areas, such as the trunk, arms, or legs, and for well-defined primary tumors. It is a simple procedure, usually outpatient, with very high cure rates: in most cases, this is sufficient.

About the Mohs surgery, Mohs, a technique that removes the tumor layer by layer, examining it under a microscope during the procedure, helps to clear up a common misunderstanding. It's not "what needs to be done always" nor the default first optionConventional excision surgery is highly curative in most cases. Mohs is one of the surgical options, depending on individual assessment, which is reserved primarily for the most delicate areas of the face (nose, eyelids, ears), for tumors that have already recurred, and for subtypes with poorly defined borders. (Peris et al., 2023)
The data from the reference trial help put things into perspective when interpreted with the necessary nuance. In a Dutch trial of selected high-risk facial basal cell carcinoma, the difference between Mohs surgery and excision was not statistically significant for primary tumors: 10-year recurrence rate of 4.41% with Mohs versus 12.21% with excision, with a p-value of 0.100; at 5 years, 2.51% versus 4.11%, p-value of 0.397. (van Loo et al, 2014)
The clear and significant benefit of Mohs appears when the tumor has recurred before, not on the first occurrence. It is worth emphasizing: these figures are for selected difficult facial cases, not for the typical low-risk basal cell carcinoma, and in all scenarios, the vast majority of patients are cured. (Mosterd et al, 2008)
A Cochrane review that gathered 52 trials and 6690 patients summarizes the logic for choosing treatment well: surgery results in the fewest recurrences; non-surgical treatments, used for low-risk basal cell carcinomas, offer slightly less protection but, in return, the skin usually ends up looking better. There is no single "best treatment": there is the best treatment for your case, and almost always with an excellent outcome. (Thomson et al, 2020)
The superficial subtype: when the scalpel can be avoided
Low-risk superficial basal cell carcinoma is the face that best responds to non-surgical options, allowing for comfortable treatments with good aesthetic results. A 3-year trial compared the three most studied non-surgical alternatives for this variant, with these tumor-free survival results. (Roozeboom et al, 2016)
- Imiquimod (immunoactivating cream): 79.7%
- The most effective non-surgical option in the superficial subtype.
- 5-fluorouracil (topical chemotherapy): 68.2%
- Intermediate result, a reasonable alternative.
- Photodynamic therapy: 58.0%
- Good aesthetic result; especially useful in the legs of older patients.
The important nuance is that the "best" treatment depends on who and where: in elderly people with a superficial leg injury, for example, the photodynamic therapy it clearly turned out to be the best option. That is why the decision is always individualized in consultation.
European guidelines also include destructive methods, such as cryotherapy (controlled freezing of the lesion) or curettage with electrocoagulation, for selected low-risk superficial basal cell carcinomas, always according to the individual assessment of the dermatologist. (Peris et al., 2023)
In particularly delicate areas, such as the eye contour, Mohs surgery serves precisely to preserve as much healthy tissue as possible, one of the reasons why it is reserved for those locations and not for typical low-risk basal cell carcinoma. (Erripi et al, 2024)
"In consultations, I often repeat one idea: basal cell carcinoma is, in the vast majority of cases, a problem with a simple solution. The question is usually not whether it can be cured, but rather what is the best way to do it in your specific case."
What if the basal cell carcinoma is advanced?
Advanced basal cell carcinoma, which has grown extensively locally or, very rarely, has spread, is uncommon and almost always the result of years of neglect. Nevertheless, and this is the central message, it now has effective treatment. If you have a recent, diagnosed basal cell carcinoma, this scenario is almost never applicable to you: The worst-case scenario is rare and, furthermore, treatable..
Biology explains why there is treatment. Most basal cells have a molecular pathway abnormally "turned on" called via Hedgehog, a pathway that is typically inactive in adults but, when disrupted, causes the tumor to grow. There are pills available that block this pathway. In the pivotal trial of vismodegib, approximately 43.1% of locally advanced basal cell carcinomas and 30.1% of metastatic cases responded, as determined by independent review. (Sekulic et al, 2012)
The final analysis of the same program confirmed durable responses, with an objective response rate of 60.31% in locally advanced disease, as assessed by the investigator. (Sekulic et al, 2017)
A second drug in the same class, sonidegib, achieved a 56.1% response rate in locally advanced disease, with an interesting clinical finding: increasing the dose does not improve efficacy but does worsen tolerability, so sometimes more of the drug is worse, not better. (Dummer et al, 2020)
A recent meta-analysis of 22 studies estimates the pooled overall response rate for this class of drugs at approximately 64.91%, confirming that even advanced cases—which are the exception—have an effective targeted treatment available. (Nguyen et al, 2023)
These drugs have predictable class effects, such as muscle spasms, hair loss, or altered taste, which the medical team manages with breaks and adjustments and which improve upon completion of treatment. And if Hedgehog pathway inhibitors fail or are not tolerated, there is a second line of treatment with immunotherapy (cemiplimab), which reactivates the patient's own defenses. (Shalhout et al, 2021)
The treatment tree has several branches, but the vast majority of patients don't even need to go up from the first one.
Can it be prevented? What follow-up do I need if one has been removed?
Yes, the risk of new basal cell carcinomas can be reduced, and Follow-up after removal is straightforward and routine.. If you've had one removed, here's the best news: detected early, new ones are easily resolved, and regular dermatological check-ups turn uncertainty into peace of mind.
The basis of prevention is sustained photoprotection: accumulated sun damage drives basal cell carcinoma, so good protection habits reduce the appearance of new lesions. If you want to learn more, I wrote a guide on best sunscreens and how to choose them.
About the nicotinamide, a form of vitamin B3, deserves to be discussed honestly, without overselling or dismissing it. In the landmark trial, nicotinamide reduced the overall incidence of non-melanoma skin cancer by 23% compared to placebo (p = 0.02); however, for basal cell carcinoma alone, the reduction was 20% and did not reach statistical significance (p = 0.12), and the benefit disappeared upon discontinuation. (Chen et al, 2015)
In organ transplant recipients, a very high-risk population, another trial found no benefit. (Allen et al, 2023)
The countervailing evidence is positive and recent. A large cohort of 33,822 patients found that nicotinamide was associated with a 141% lower risk of skin cancer, a figure that rises to a 54% reduction when treatment is started after the first skin cancer. Breglio et al, 2025
Practical conclusion for the reader: In people who have already had injuries, nicotinamide is a reasonable and safe prevention option, the sooner it is started, the better, and always according to the individual assessment of your dermatologist. I develop this in detail in the article about Nicotinamide and skin cancer.
Regarding follow-up, guidelines recommend periodic skin checks for individuals with high-risk basal cell carcinoma, multiple lesions, or genetic predisposition, always tailored to each case. It is not distressing surveillance: it is a calm routine, similar to a regular check-up, whose objective is precisely to catch any new lesion early and easily. (Peris et al., 2023)
If you've had a basal cell carcinoma removed, the realistic outlook for your future is good: with sun protection, simple check-ups, and nicotinamide prevention if appropriate, most of my patients lead absolutely normal lives and stop thinking of it as a problem. Acting in time, which is usually the case, turns this tumor into what it really is: a minor issue with a very good prognosis.
Frequently Asked Questions about Basal Cell Carcinoma
Basal cell carcinoma is malignant.
What happens if I don't take it off? Is it dangerous?
Does basal cell carcinoma metastasize?
How does a basal cell carcinoma start? What are the first symptoms?
What is the treatment of choice? Is there a cream treatment?
What is Mohs surgery and when is it performed?
I had a basal cell carcinoma removed. Will I get more? What follow-up do I need?
Do you have a skin lesion that worries you? A timely assessment is usually simple and, almost always, reassuring. Choose the option that best suits you.
References
- Kim DP et al. Basal Cell Carcinoma Review. Hematology/Oncology Clinics of North America, 2019. PubMed
- Peris K et al. Diagnosis and treatment of basal cell carcinoma: European consensus-based interdisciplinary guidelines. European Journal of Cancer, 2023. PubMed
- García Ruiz R et al. Basal cell carcinoma: incidence and trends in Valencia. Dermo-Syphilographic Records, 2024. Dermo-Syphilographic Records
- Kappelin J et al. Incidence and trends of basal cell carcinoma in Sweden: a population-based registry study. Br J Dermatol, 2022. British Journal of Dermatology
- Conte S et al. Clinical and Molecular Features of Morpheaform Basal Cell Carcinoma: A Systematic Review. Curr Oncol, 2023. Current Oncology
- Lallas A et al. Accuracy of dermoscopic criteria for discriminating superficial from other subtypes of basal cell carcinoma. Journal of the American Academy of Dermatology, 2014. JAAD
- Reiter O et al. The diagnostic accuracy of dermoscopy for basal cell carcinoma: a systematic review and meta-analysis. Journal of the American Academy of Dermatology, 2019. JAAD
- Álvarez-Salafranca M et al. Dermoscopy of basal cell carcinoma: an updated review. Dermo-Syphilographic Records, 2021. Dermo-Syphilographic Records
- Amici JM et al. Clinical factors predictive for histological aggressiveness of basal cell carcinoma: a prospective study of 2274 cases. Annals of Dermatology and Venereology, 2021. PubMed
- van Loo E et al. Surgical excision versus Mohs' micrographic surgery for basal cell carcinoma of the face: 10-year follow-up. European Journal of Cancer, 2014. European Journal of Cancer
- Mosterd K et al. Surgical excision versus Mohs' micrographic surgery for primary and recurrent basal-cell carcinoma of the face: 5-year follow-up. Lancet Oncology, 2008. The Lancet Oncology
- Thomson J et al. Interventions for basal cell carcinoma of the skin. Cochrane Database of Systematic Reviews, 2020. Cochrane Library
- Roozeboom MH et al. Three-year follow-up of photodynamic therapy vs. imiquimod vs. fluorouracil for superficial basal cell carcinoma. Journal of Investigative Dermatology, 2016. Journal of Investigative Dermatology
- Erripi K et al. Mohs micrographic surgery for periocular basal cell carcinoma. Acta Derm Venereol, 2024. PubMed
- Sekulic A et al. Efficacy and Safety of Vismodegib in Advanced Basal-Cell Carcinoma (ERIVANCE). New England Journal of Medicine, 2012. New England Journal of Medicine
- Sekulic A et al. Long-term safety and efficacy of vismodegib in advanced basal cell carcinoma: final update of the ERIVANCE BCC study. BMC Cancer, 2017. BMC Cancer
- Dummer R et al. Long-term efficacy and safety of sonidegib in advanced basal cell carcinoma: 42-month BOLT analysis. Br J Dermatol, 2020. British Journal of Dermatology
- Nguyen A et al. Efficacy and Safety of Sonic Hedgehog Inhibitors in Basal Cell Carcinomas: An Updated Systematic Review and Meta-analysis. Am J Clin Dermatol, 2023. American Journal of Clinical Dermatology
- Shalhout SZ et al. Systemic Therapies for Advanced Basal Cell Carcinoma. Current Oncology Reports, 2021. PubMed
- Chen AC et al. A Phase 3 Randomized Trial of Nicotinamide for Skin-Cancer Chemoprevention (ONTRAC). New England Journal of Medicine, 2015. New England Journal of Medicine
- Allen NC et al. Nicotinamide for Skin-Cancer Chemoprevention in Transplant Recipients (ONTRANS). New England Journal of Medicine, 2023. New England Journal of Medicine
- Breglio KF et al. Nicotinamide for Skin Cancer Chemoprevention. JAMA Dermatology, 2025. JAMA Dermatology