Melanonychia, that dark line that appears on a nail, is one of the reasons for consultation that generates most concern among my patients. The good news is that the vast majority of these pigmented bands are benign. Subungual melanoma accounts for only 1.9% of all melanomas.. [(Tsiogka et al., 2024)].
Some time ago, I gave a talk to a group of patients about moles and melanoma on the nails. Seeing the interest and concern on their faces, I realized the importance of spreading this knowledge to all my patients and readers.
My name is Sebastian Podlipnik and I am Dermatologist at the Melanoma and Skin Cancer Unit of Hospital Clínic de Barcelona. During my years of experience I have evaluated many patients with melanonychia and I can tell you that knowing how to differentiate when a line on the nail requires attention and when you can rest easy is critical.
What is melanonychia and why do dark lines appear on the nails?
Melanonychia is a clinical sign, not a disease. It refers to the presence of a brown or black pigmented band running longitudinally across the nail. When this band runs from the base to the free edge of the nail, it is called longitudinal melanonychia.
The cells that produce the pigment (melanocytes) are found in the nail matrix, the most proximal area from which the nail plate grows. When these melanocytes are activated or proliferate, the pigment adheres to the nail and moves towards the free edge as the nail grows. It is like a conveyor belt that leaves a continuous mark.
- Longitudinal melanonychia
- Pigmented band that runs longitudinally along the nail, from the base to the free edge. It is not a diagnosis by itself, but a clinical sign that may correspond to benign causes (the majority) or, in a small percentage, to melanoma.
What do moles look like on the nails?
Nail moles (nail nevi) are very stable lesions that do not change significantly over time. They appear as a regular, usually narrow, well-demarcated, homogeneously colored band of pigment affecting a single nail.
With dermoscopy (a special microscope used by dermatologists), moles show a pattern of parallel lines regular in color and thickness. This ordered pattern is the key that allows us to differentiate a benign mole from a suspicious lesion. Regular parallel lines on dermatoscopy indicate benignity..
What signs should lead one to suspect melanoma of the nail?
Nail melanoma differs from benign moles in that it presents progressive changes, irregularity and extension of the pigment beyond the nail. Although it is a rare form of skin cancer, If it is detected early, early detection is essential because the prognosis is greatly improved with early diagnosis.
ABCDEF rule for nail melanoma
Dermatologists use the ABCDEF rule as a guide to evaluate pigmented nail bands. [(Levit et al., 2000)].
- A (Age): Nail melanoma is more frequent between the ages of 50 and 70, and in people of high phototypes (African Americans, Asians, Hispanics).
- B (Band): Brown or black band more than 3 mm wide with irregular or fuzzy edges
- C (Change): Any rapid change in color, size or shape of the band
- D (Digit): The thumb and the first toe are most frequently affected
- E (Extension): Pigmentation extending to the nail fold or periungual skin (Hutchinson's sign)
- F (Family): Personal or family history of melanoma
A study that evaluated 84 melanonychia biopsies found that a band greater than 40% of the nail width is the best predictor of melanoma. (p=0,002). [(Ko et al., 2019)]
Progressive changes
Benign nail moles are very stable. One of the first signs of melanoma is progressive change: the band becomes wider, darker or changes shape within weeks or months. Nail melanoma grows, benign mole remains stable.
Triangular shape of the pigmented band
If a lesion grows rapidly, the newer pigment (near the matrix) will be wider than the older pigment (at the free edge). This generates a characteristic triangular shape which is an important warning sign.
Other important signs
- Greater than ⅓ thickness of the nail: If the pigment band occupies more than one-third of the total width of the nail
- Pigmentation beyond the nail: When the brown pigmentation spreads to the skin surrounding the nail
- Hutchinson's sign: Pigmentation affecting the proximal nail fold, one of the most specific signs of nail melanoma.
- Destruction of the nail plate: When the nail is broken, deformed or lifted up
Consult your dermatologist if you notice
- A new dark band on a single nail that you had not noticed before
- A progressive change in the width, color, or shape of an existing band
- Pigmentation spreading to the skin around the nail
- Destruction or deformation of the nail plate together with pigmentation.
Benign vs. malignant melanonychia: how to tell the difference?
Most melanonychia are benign. A dermoscopic study found that the most useful signs to suspect malignancy are band asymmetry (OR 34.0), Hutchinson's sign (OR 18.2) and the presence of multiple colors (OR 11.6). Band asymmetry is the strongest predictor of nail melanoma. [(Ohn et al., 2018)]
| Feature | Benign melanonychia | Suspected melanoma |
|---|---|---|
| Bandwidth | Narrow (<3 mm) | Wide (>3 mm or >40% of width) |
| Edges | Regular and well-defined | Irregular and diffuse |
| Color | Homogeneous (single tone) | Heterogeneous (multiple tones) |
| Evolution | Stable over time | Progressive changes |
| Hutchinson's sign | Absent | Present |
| Number of nails | It may affect one or more | Almost always a single nail |
He recalls a 62-year-old patient who came for consultation because his wife had noticed that the dark line on his thumb was widening. He had had it for years and had never given it any thought. Dermoscopy showed an irregular pattern and it eventually turned out to be melanoma in situ. Detection was timely and treatment was conservative, with no need to amputate the finger.
"Most dark lines on the nails are benign. But if you notice a change, don't let it go. Consulting early can make all the difference."
Dr. Sebastian Podlipnik
Do you have a spot on your nail that worries you?
I can evaluate it with dermoscopy and give you an accurate diagnosis.
Melanonychia in children: should I be concerned?
In children, longitudinal melanonychia is almost always benign. A meta-analysis of 1,391 pediatric patients found that 86.3% corresponded to benign nevi. No invasive melanoma has been reported in children with melanonychia.. [(Tsai et al., 2024)].
This is very reassuring for parents who come to my office concerned about a dark line on their child's nail. In the vast majority of cases, the correct approach is to perform periodic follow-up with digital dermoscopy, without the need for biopsies or surgery.
One detail that I always explain to parents: melanonychia in children can change appearance during growth and this does not necessarily indicate malignancy. The important thing is that these changes are evaluated by a dermatologist with experience in nail lesions.
Are there other causes of dark nail lines?
Many conditions can produce pigmented bands on the nails in addition to moles and melanoma. Broadly speaking, the causes fall into two groups: melanocytic activation (melanocytes produce more pigment than normal) and melanocytic proliferation (the number of melanocytes increases, as in moles and melanoma).
A key difference is that melanocytic activation usually affects several nails at once, whereas moles and melanoma typically affect a single nail. If several nails are affected, the cause is usually benign..
Drug-induced melanonychia
Several medications can cause melanonychia as a side effect. The most frequent are:
- Chemotherapy: Cyclophosphamide, doxorubicin, 5-fluorouracil
- Antiretrovirals: Zidovudine (AZT), the most known to cause melanonychia.
- Antimalarials: Chloroquine, hydroxychloroquine
- Others: Minocycline, psoralens (used in phototherapy)
Melanonychia in dark skins
In people with high phototypes (dark skin), melanonychia is frequent, physiological and does not require treatment. It can affect multiple nails and does not require any treatment. However, it is important to have a dermatologist confirm that it is racial melanonychia and not another cause.
There are also other common causes of melanocytic activation such as pregnancy, repeated trauma (nail biting, narrow shoes), infections, lichen planus, psoriasis, Addison's disease and hyperthyroidism.
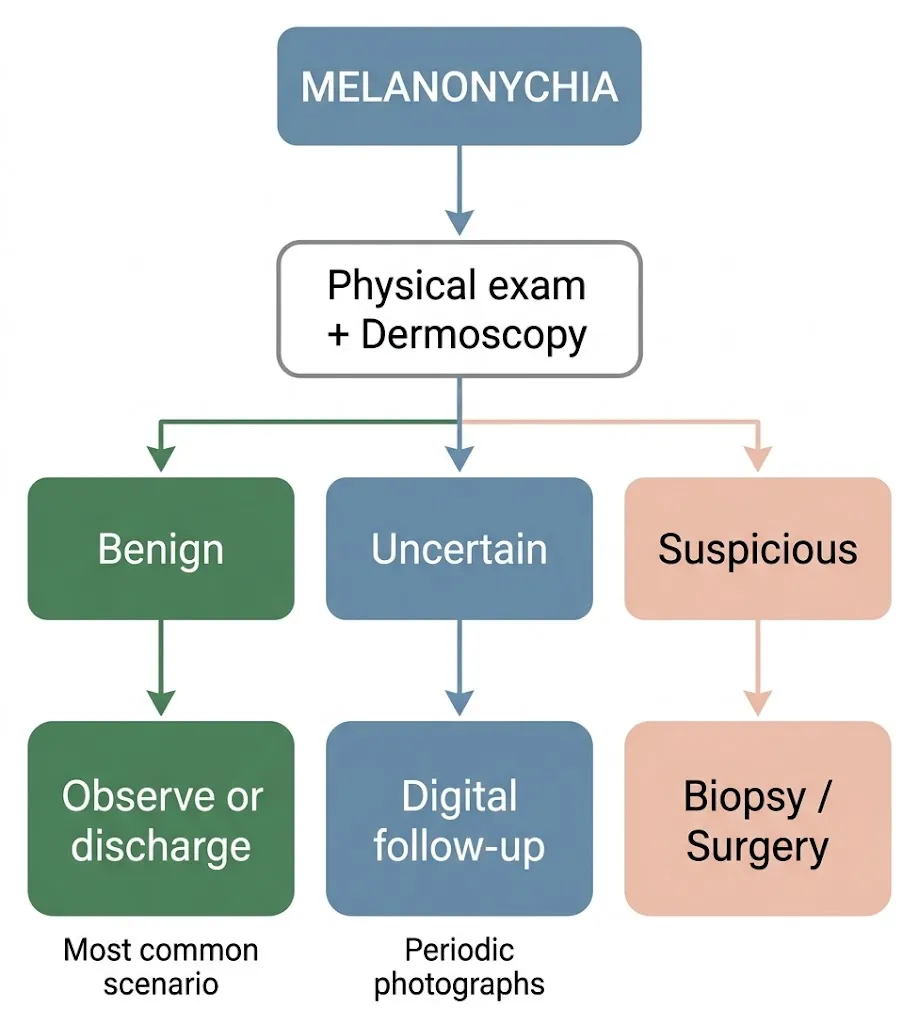
What do we do in the dermatological practice when we see a melanonychia?
To properly evaluate a melanonychia, we follow a systematic three-step process that allows us to make the best decision for each patient. Excisional biopsy of the nail matrix remains the gold standard for definitive diagnosis, but not all melanonychia require biopsy. [(Ricardo et al., 2025)].
1. Physical examination
The first thing I do is a complete physical examination of all your nails, both fingernails and toenails. I evaluate for deformity, whether the melanonychia affects one or more nails, and analyze the color, shape and size of the band. In addition, I review your medical history to identify conditions or medications that may explain the pigmentation.
2. Dermatoscopy (onychoscopy)
I then use the dermatoscopy, I use a special microscope that allows me to examine the band pattern in great detail. The most useful dermatoscopic signs to suspect malignancy are asymmetry, the presence of multiple colors and irregularity of the lines. [(Ohn et al., 2018)]
One piece of data that reflects the complexity of this diagnosis: a study of 152 dermatologists found that the overall accuracy for diagnosing nail melanoma was 46-55%, regardless of experience level. [(Di Chiacchio et al., 2010)]. This reinforces the importance of combining clinical evaluation with dermoscopy and, when in doubt, digital follow-up or biopsy.
3. Take a behavior
After clinical and dermatoscopic evaluation, there are three possible scenarios:
- Clearly benign lesion: We do nothing or discharge. This is the most frequent scenario
- Doubtful injury: We perform digital follow-up with periodic photos to detect changes over time. We can also request a partial biopsy (nail clipping) to get more information.
- Suspicious lesion of malignancy: We directly propose an excisional biopsy or surgery to remove and analyze the entire lesion.
Treatment of nail melanoma: amputation is no longer always performed
The treatment of nail melanoma has changed greatly in recent years. Surgical management has evolved from aggressive amputations to conservative approaches that preserve the digit. [(Zhang et al., 2021)].
For in situ (confined to the epidermis) or minimally invasive melanomas, the current trend is for conservative functional surgery, which removes the lesion while preserving the toe. Amputation is reserved only for cases with bone invasion or advanced disease. [(Darmawan et al., 2022)].
But most melanonychias do not require surgery. If after the evaluation we conclude that the lesion is benign, the attitude is simply to observe or perform a periodic follow-up. Only when there is suspicion of malignancy do we consider surgical treatment.
Early diagnosis is what makes the difference in prognosis. A melanoma detected in situ has an excellent prognosis and can be treated conservatively. If you want to know more about how it is classified, I explain it in my article on the prognosis of melanoma.
Frequently asked questions about melanonychia
Is melanonychia cancer?
No. Melanonychia is a clinical sign that describes the presence of a pigmented band on the nail. The vast majority of melanonychia are benign and are due to moles, melanocytic activation by drugs, trauma or racial factors. Only a very small percentage corresponds to melanoma (1.9% of all cutaneous melanomas).
Is it normal to have a black line on the nail?
It can be completely normal, especially in people with dark skin, where longitudinal melanonychia is physiological and frequent. It may also be due to minor trauma or certain medications. However, if it is new, affects a single nail or is changing, it should be evaluated by a dermatologist.
When should I go to a dermatologist for a spot on the nail?
You should consult if the band is new and you have not noticed it before, if it is changing (widening, darkening or changing shape), if the pigment extends to the skin around the nail, or if the nail is deformed. If you have any doubts, it is always best to ask for advice to put your mind at ease.
Can nail melanoma be cured?
Yes, especially when detected in early stages. Melanoma in situ has an excellent prognosis and can be treated with conservative surgery, without the need to amputate the finger. That is why I insist on the importance of not delaying consultation in the event of any suspicious change.
Is melanonychia in children dangerous?
In the vast majority of cases, no. A meta-analysis with 1,391 children found that 86.3% were benign nevi and no invasive melanoma was reported in pediatric age. Even so, it is recommended that a dermatologist evaluate the lesion and perform periodic follow-up.
Consultation with a melanoma specialist
If you have a pigmented nail band that concerns you, a dermatology consultation can give you peace of mind or, if necessary, an appropriate follow-up plan. Most of the time you'll leave the consultation knowing that everything is fine. And if not, you will have taken the most important step: detect in time. If you want to learn more about how to identify malignant moles or know the types of skin cancer, I invite you to read my guides. You may also be interested in learning more about the moles on soles of feet and palms, another special localization of acral melanoma.
Do you want me to evaluate your melanonychia?
I can help you determine if you need follow-up or treatment.