In early July 2020, I submitted my doctoral dissertation to the University of Barcelona to be reviewed in front of a panel of experts. The 160+ page document was the culmination of about four years of effort. At this stage I learned a great deal about the specialty of dermatology and confirmed that I am passionate about what I do. The best part is that I feel that the results of the studies performed will have a real impact on the prognosis of patients with melanoma.

Submit thesis in COVID period.
One of the great difficulties I had was to prepare the final details of my doctoral thesis during the months of COVID quarantine. In addition, the University asked me to do it telematically, which I was a little reluctant to do at first. However, something happened that I never thought about, and that is that I was able to share this moment with all my friends and family from a distance. In the following video I leave you the presentation of the defense of my doctoral thesis, or if you prefer I will leave a summary below in this post. Now, for the very motivated ones I will leave you this one link where you can download it.
Dissertation Tribunal
- President: Vicente García-Patos (orcid), Head of the Dermatology Department of the Vall d'Hebron University Hospital.
- Secretary: Aleix Prat (Linkedin), Head of the Oncology Department of the Hospital Clínic de Barcelona
- Vocal: Eduardo Nagore (Linkedin), Head of Section in the Dermatology Service of the Valencian Institute of Oncology Foundation (IVO).
- Thesis director: Susana Puig (linkedin), Head of the Dermatology Department of the Hospital Clínic de Barcelona.
What impact does melanoma have on our society?
Melanoma accounts for only 5% of all melanomas. skin cancersHowever, it is responsible for more than 90% of deaths associated with skin neoplasms. The most worrying aspect is that its incidence continues to increase despite major population prevention campaigns. Consequently, the increase in prevalent cases has led to an overload of care in several hospital services.
In addition, the recent introduction of new target treatments and immunotherapy in melanoma has led to improved survival of metastatic patients and a lower relapse rate in high-risk patients undergoing adjuvant therapy.
Why is follow-up of melanoma patients important?
A fundamental part of patient care is the staging of melanoma to define the patient's risk of relapse, and thus define the follow-up required in each case. In this doctoral thesis we hypothesized that defining the optimal follow-up schedule in the patients with melanoma and identify high-risk melanoma tumors at high risk.The use of new prognostic and genetic tests makes it possible to detect subclinical metastases and initiate treatment early, in order to improve patient survival and optimize hospital resources.
Objectives of my doctoral thesis
- To describe the diagnostic cost-effectiveness of currently used follow-up schemes in patients with high- and low-risk melanoma according to the American Joint Committee of Cancer (AJCC).
- To conduct a cost-effectiveness study of the follow-up regimen used in melanoma.
- To analyze the diagnostic accuracy of gene expression profiling in the detection of melanoma recurrence.
- To analyze the MC1R gene variants in the prognosis of patients and to evaluate if there are differences between sexes.
To meet all these objectives, 5 studies were designed.
Study 1: assessment of the efficacy of an intensive follow-up protocol
In the first study published in The Journal of the American Academy of Dermatology, we conducted a retrospective cohort study over a 10-year period. We wanted to establish the diagnostic yield of different components of an intensive follow-up protocol in the early detection of metastases. In this cohort metastases were detected in a decreasing manner by axial tomography (CT) of the chest, abdomen and pelvis in 48.3%, physical examination in 23.7%, patient self-exploration in 17.8%, brain magnetic resonance imaging (MRI) in 7.6% and tumor markers (S100B and/or MIA) in 2.5%. We were able to conclude that intensive follow-up with serial imaging studies allows detection of metastases asymptomatically in most patients.
Study 2: cost-effectiveness of follow-up protocols
In the second study published in The British Journal of DermatologyWe conducted an economic study to evaluate whether CT of the chest, abdomen and pelvis, and brain MRI are cost-effective in an intensive follow-up protocol in patients at high risk of recurrence. The economic analysis showed that CT was cost-effective during the first 4 years of follow-up, with a cost-effectiveness ratio of €4,710.70 - €14,437.10 per patient. In addition, brain MRI was cost-effective during the first year of follow-up with a cost-effectiveness ratio of € 14,090.00 per patient. From the findings obtained in this study we can conclude that incorporating these changes to the current follow-up guidelines could improve the cost-effectiveness of the follow-up protocols.

Study 3: Diagnostic cost-effectiveness of imaging tests in patients at low risk of recurrence.
In the THIRD JOB published in The European Journal of Cancer we studied the cost-effectiveness of complementary tests in patients at low risk of AJCC recurrence. For this purpose, we used a retrospective cohort model to compare a follow-up protocol based on abdominal and regional lymph node ultrasound with a clinical follow-up protocol based on periodic visits to the specialist's office. We were able to conclude that abdominal and locoregional nodal ultrasound for the follow-up of low-risk patients does not improve prognosis or disease-free time in patients with AJCC stage IB and IIA.

Study 4: Tumor gene expression profiles for predicting prognosis in melanoma
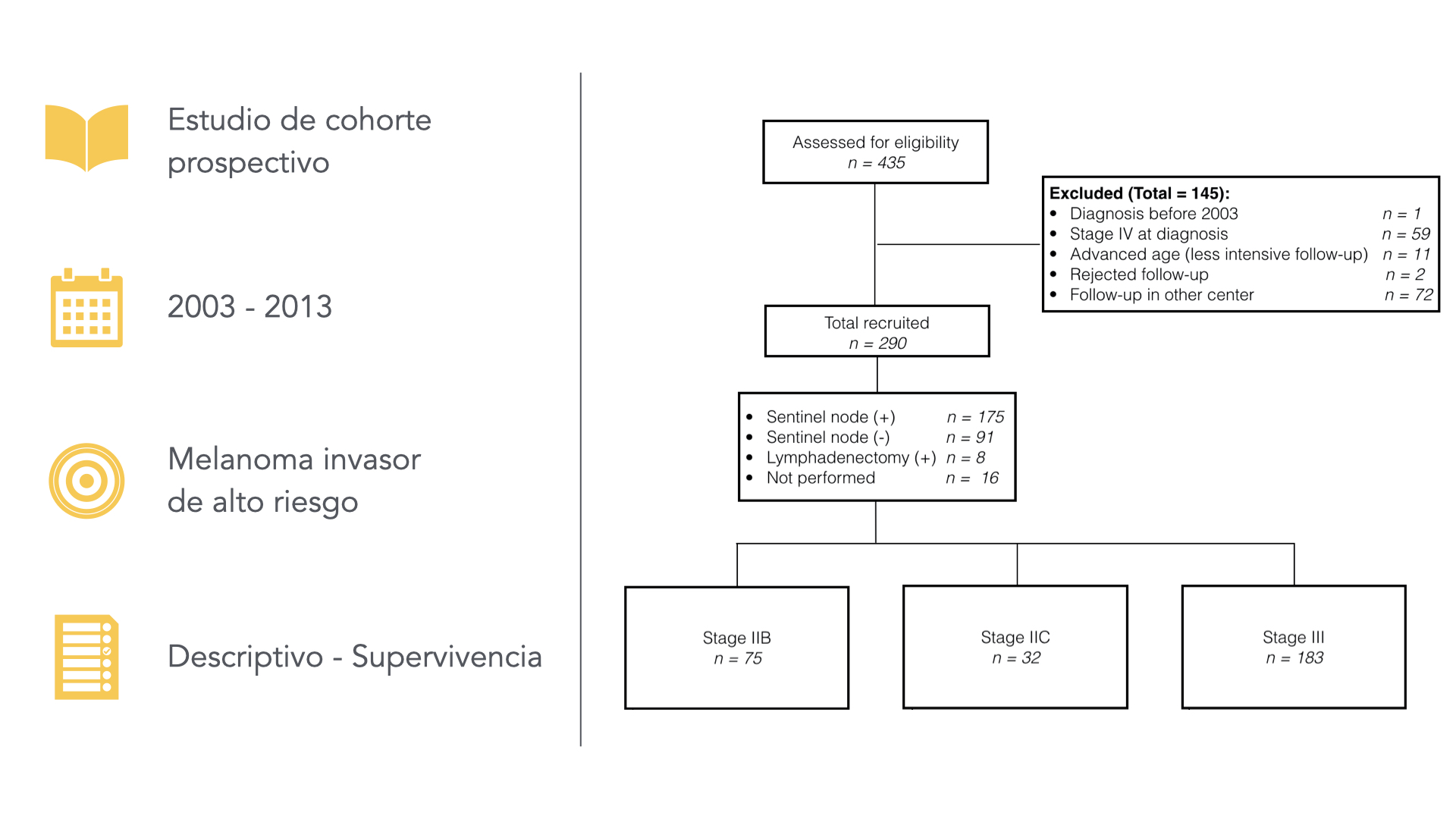
In the fourth study published in The Journal of the European Academy of Dermatology and Venereology We assessed the usefulness of a new gene expression profile on the primary tumor, based on 31 genes, to classify those patients with a higher risk of recurrence. A prospective multicenter design was used for its development, including 5 tertiary care centers in Spain. Patients with AJCC stages IB-IIC were consecutively recruited from April 2015 to December 2016. During the follow-up time we observed that seven patients (8.1%) presented relapses, all in group 2 or high risk. Multivariate analysis showed that this test was an independent prognostic factor with a hazard ratio (HR) of 18.82 (1.81-2,549.76; P= 0.01). Derived from the data obtained in this study, we observed that this gene expression profile is able to correctly classify different risk groups of melanoma patients and better define the prognosis of each patient.

Study 5: Patient genetics differentially influences melanoma prognosis in men and women.
Finally, in the fifth job of this thesis published in The British Journal of Dermatology We assessed whether the variants of the gene for MC1R confer a different prognosis in men and women. For this purpose, we used a retrospective cohort model including more than 1,341 melanoma patients who had undergone genetic screening. We then stratified both cohorts by sex (P-value for interaction 0.004) and could observe that MC1R variants conferred a protective effect in women but this survival benefit was not observed in men. We believe that future survival studies should take these considerations into account and include sex in their analyses.

Conclusions of the doctoral thesis and prognostic implication in melanoma.
Thanks to our work, we have been able to advance our knowledge of the benefits of imaging techniques in the follow-up of patients with high-risk melanoma, and to determine in which periods they are cost-effective. On the other hand, we have established that in low-risk patients according to the AJCC, imaging techniques do not provide benefits, unless we are able to identify high-risk subgroups by gene expression profiling and be able to offer these patients a different follow-up (similar to high-risk patients). Finally, the discovery of germline genetic differences between men and women raises the question of whether we should adapt follow-up protocols based on sex and hormonal status. All these studies bring us one step closer to improving the prognosis in melanoma.